
OHSS or Ovarian Hyperstimulation Syndrome- Symptoms, Diagnosis and Management and Prevention
Ovarian hyperstimulation syndrome (OHSS) is a complication of Fertility treatment, which uses pharmacological agents to cause ovarian stimulation to increase the number of oocytes and therefore the number of embryos available during assisted reproductive technology (ART). In a minority of women undergoing treatment, the ovarian response exceeds that aimed for and results in a clinical condition with a specific pathophysiology.
Ovarian hyperstimulation syndrome (OHSS) is by far the most serious complication of ovulation induction which results in a wide spectrum of clinical and laboratory signs and symptoms. It occurs as a hyper response to ovulation induction in patients undergoing assisted reproduction. It is known that the incidence of OHSS varies between different types of fertility treatment, with treatments involving greater degrees of ovarian stimulation being associated with a higher incidence.
The overall incidence is 2-3%.
Classification of OHSS
The diagnosis is based on clinical criteria. It is therefore very important to have a classification, based on the symptoms.
Ovarian hyperstimulation syndrome has been classified into various stages and grades according to the clinical symptoms, signs, ultrasonographic findings and laboratory parameters.
In general, mild and moderate form of OHSS can be treated expectantly on out-patient department basis.
Those with severe form should be admitted and those with critical OHSS are best managed in consultation with other specialist in an intensive care setting.
Fortunately, with the current treatment protocols, the incidence of severe and critical OHSS is negligible.
The key principles of OHSS management therefore are early recognition and the prompt assessment and treatment of women with moderate or severe OHSS.
Types of Ovarian Hyperstimulation Syndrome
- Early: Within 5-7 days of hCG trigger
- Late: Observed once pregnancy occurs
Symptoms of OHSS:
Based on the severity OHSS symptoms are categorized into three types:
- Mild OHSS
- Feeling Bloated and
- Swollen Abdomen
- Increased waist size with mild discomfort ,
- That may be accompanied with Nausea.
- Moderate OHSS
- Moderate abdominal pain
- Nausea ± vomiting
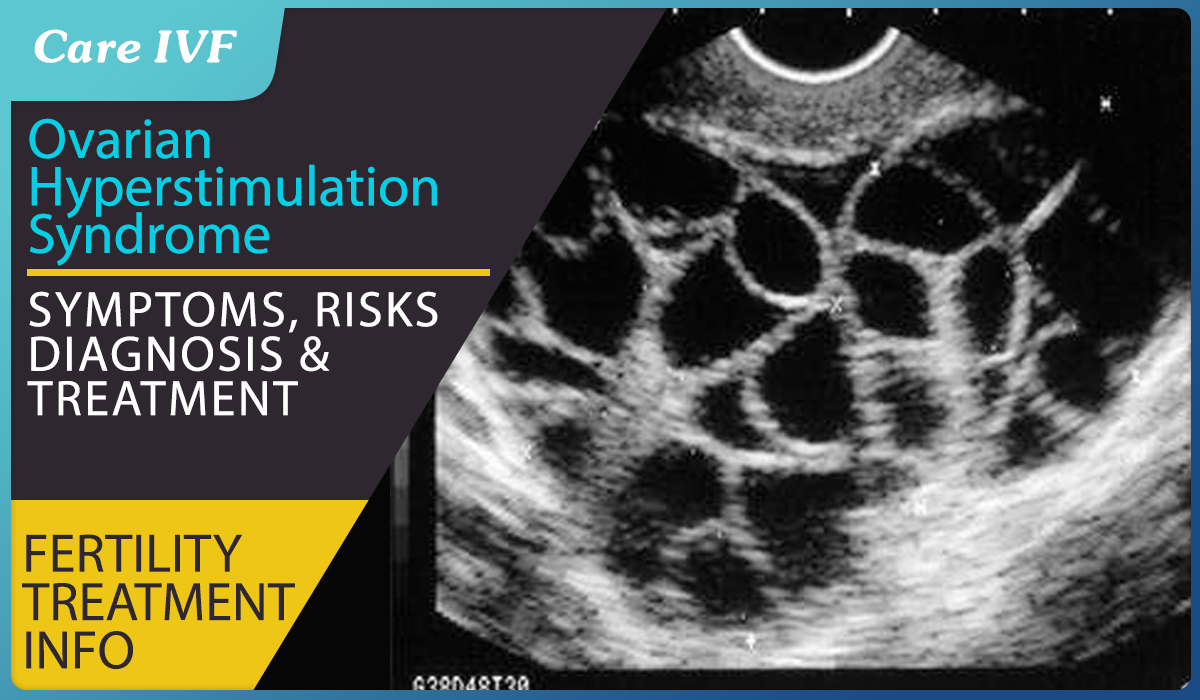
- Ulrasound evidence of Fluid (ascites) buildup in abdomen
- Reduced urination
- Severe OHS
- Severe abdominal pain and nausea,
- Extreme thirst and dehydration,
- Reduced urination with dark coloration of urine,
- Breathing difficulty,
- Swollen legs due to blood clots,
- Enlarged abdomen.
- Rapid increase in body weight within 24 hours
Risk factors for Ovarian Hyperstimulation Syndrome
Certain patient and cycle characteristics increase the risk of OHSS; women with a previous history of OHSS, polycystic ovary syndrome, increased antral follicle count (AFC) or high levels of anti-Müllerian hormone (AMH) are at an increased risk of OHSS.
Various factors have been identified to help define patients at high risk of ovarian hyperstimulation syndrome:
- Age less than 30 years
- Polycystic ovarian disease (PCOD), especially lean PCO
- Serum estradiol (E2) level greater than 3,500 pg/mL
- High baseline Anti-Mullerian hormone(AMH) levels
- High antral follicle count on D2/D3 scan
- Previous history of OHSS
- Large number of small follicles (8-12 mm) during stimulation
- Use of hCG for trigger and/or luteal support
- Large number of oocytes retrieved (>25)
How is OHSS diagnosed?
The diagnosis of OHSS is made on clinical grounds (Case study 1 & 2)
The typical patient presents with abdominal distension and discomfort following the trigger injection used to promote final follicular maturation prior to oocyte retrieval.
There may be a preceding history of an excessive ovarian response to stimulation, but the absence of such a history does not rule out a diagnosis of OHSS. The time of presentation following trigger injection divides patients into two groups:
Diagnosing Early and late OHSS
Early’ OHSS usually presents within 7 days of the hCG injection and is usually associated with an excessive ovarian response. ‘Late’ OHSS typically presents 10 or more days after the hCG injection and is usually the result of endogenous hCG derived from an early pregnancy. The preceding ovarian response in these women may be unremarkable. Late OHSS tends to be more prolonged and severe than the early form.
Your physician will following the following steps for diagnosis of OHSS:
Take detailed history from a woman suspected to be suffering from OHSS
History
- Time of onset of symptoms relative to trigger
- Medication used for trigger (hCG or GnRH agonist)
- Number of follicles on final monitoring scan
- Number of eggs collected
- Were embryos replaced and how many?
- Polycystic ovary syndrome diagnosis?
Symptoms
- Abdominal bloating
- Abdominal discomfort/pain, need for analgesia
- Nausea and vomiting
- Breathlessness, inability to lie flat or talk in full sentences
- Reduced urine output
- Leg swelling
- Vulval swelling
- Associated comorbidities such as thrombosis
Examination and investigation of women with suspected OHSS
General Examination: assess for dehydration, oedema (pedal, vulval and sacral); record heart rate, respiratory rate, blood pressure, body weight
Abdominal Examination: assess for ascites, palpable mass, peritonism; measure girth
Respiratory Examination: assess for pleural effusion, pneumonia, pulmonary oedema
Investigations:
- Full blood count
- Haematocrit (haemoconcentration)
- C-reactive protein (severity)
- Urea and electrolytes (hyponatraemia and hyperkalaemia)
- Serum osmolality (hypo-osmolality)
- Liver function tests (elevated enzymes and reduced albumin)
- Coagulation profile (elevated fibrinogen and reduced antithrombin)
- hCG (to determine outcome of treatment cycle) if appropriate
- Ultrasound scan: ovarian size, pelvic and abdominal free fluid. Consider ovarian Doppler if torsion suspected
Other tests that may be indicated
- Arterial blood gases
- D-dimers
- Electrocardiogram (ECG)/echocardiogram
- Chest X-ray
- Computerised tomography pulmonary angiogram (CTPA) or ventilation/perfusion (V/Q) scan
What are the steps a doctor takes for prevention of OHSS
The primary way of preventing OHSS is identification of a high-risk patient. The patients who are most prone to develop OHSS have certain epidemiologic, hormonal and ultrasonographic characteristics that should be at the back of the mind of every clinician.
A typical patient is usually young, with lean habitus and PCOD-like hormonal composition, and a pathognomic necklace sign on ultrasonography.
During ovarian stimulation, if a patient has very high E2 levels in range of 4,000-6,000 pg/mL and multiple small, intermediate follicles are seen on sonography, the clinician should be at high alert.
Whenever a patient is at high risk, hCG trigger should be withheld or GnRH agonist trigger should be used.
OHSS management
Since the pathogenesis of OHSS is not clearly elucidated treatment remains largely empirical.
In patients having mild to moderate OHSS, bed rest, abundant liquid intake and analgesics is the first-line of treatment..
The symptoms of intravascular volume depletion and hyponatremia can be treated by balanced salt solution.
If there is Massive Ascitis and hemoconcentration, it means that OHSS is in the severe phase and hospitalization with intravenous (IV) fluid therapy is essential.
Article Tags
About the author
Also Read



Leave a Comment